

 中 文
中 文
Aging Population and Aesthetic Demands Propel CAD/CAM Market to $2.40 Billion Milestone in 2025
2025-10-15
2026-03-22
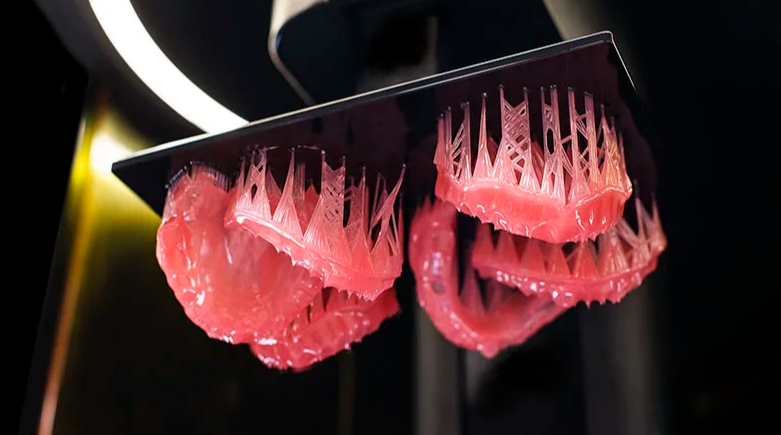
In North American dental practices, the rapid adoption of 3D printed photopolymer resins for denture bases has transformed removable prosthetics. These light-cured liquid resins enable same-day or next-day fabrication with superior precision. However, their biocompatibility hinges on controlling residual monomers—unreacted acrylate or methacrylate compounds that can leach into oral tissues. With FDA Class II clearance required for intraoral devices in prolonged mucosal contact (>30 days), clinics must prioritize evidence-based post-processing to meet ISO 10993 standards and protect patients from potential cytotoxicity, sensitization, or irritation.
This guide provides concise, data-driven clinical key points for North American practices transitioning to 3D printed resins, focusing on real-world biocompatibility metrics, FDA 510(k) pathways, and practical risk mitigation—without hype or brand references.
Photopolymer resins consist of monomers, oligomers, photoinitiators, and additives that cross-link under UV light during layer-by-layer printing. Incomplete polymerization leaves residual monomers (e.g., methyl methacrylate derivatives) that can elute over time. These leachables are the primary source of cytotoxicity in early or improperly processed prints.
Studies using high-performance liquid chromatography (HPLC) show that residual monomer content varies significantly with post-processing. One in-vitro analysis found methyl methacrylate elution in 3D printed denture bases was significantly lower than in milled alternatives when optimized washing and curing protocols were followed. Post-processed 3D printed resins exhibited no detectable cytotoxicity in cell viability assays, with monomer release levels too low to affect cell cycle distribution or cause irritation.
In contrast, uncured or minimally processed resins can release higher levels of leachables, leading to mucosal inflammation or allergic responses in sensitive patients. Water sorption and solubility also influence long-term elution, but FDA-cleared resins consistently meet ISO 20795-1 mechanical and biocompatibility thresholds when properly handled.
Under FDA regulations, 3D printed denture base resins are classified as Class II devices (21 CFR 872.3760). They require 510(k) premarket notification demonstrating substantial equivalence to predicate devices, supported by comprehensive biocompatibility testing per ISO 10993-1. Key required evaluations include:
Health Canada aligns closely, often accepting FDA-cleared devices with additional labeling for permanent mucosal contact. Non-compliant resins cannot be marketed or used for patient devices in the US or Canada. Manufacturers must validate specific printing, washing, and post-curing parameters; deviation constitutes off-label use and voids clearance.
Clinics bear responsibility for following manufacturer-validated workflows. Proper post-processing—typically 10–20 minutes IPA or specialized wash followed by extended UV post-curing (≥30 minutes at recommended wavelength and intensity)—reduces residual monomers to safe levels, often below detection thresholds in HPLC testing.
| Aspect | Traditional Heat-Cured PMMA | Optimized 3D Printed Photopolymer Resins | Clinical Implication for Safety |
|---|---|---|---|
| Residual Monomer Levels | Higher initial elution (MMA dominant) | Significantly lower with proper post-processing | Lower risk of irritation in 3D |
| Cytotoxicity (ISO 10993-5) | Generally low after full cure | No cytotoxicity in validated protocols | Equivalent or better in 3D |
| Leaching Duration | Peaks early, declines over weeks | Minimal after 24–48 hours post-cure | Faster stabilization in 3D |
| Sensitization Risk | Rare but documented | Negligible when ISO-compliant | Reduced allergic potential |
| FDA Pathway | Long-established predicates | Requires specific 510(k) for each resin | Must verify clearance status |
| Post-Processing Dependency | Flasking/heat cycle inherent | Critical (wash + UV cure) | Non-negotiable for 3D safety |
Data from multiple in-vitro studies confirm that, when post-processed correctly, 3D printed resins demonstrate superior or comparable biocompatibility profiles, with lower overall monomer release than some conventional methods

Phase 1: Audit & Selection (Weeks 1–4) Review current resin inventory and confirm 510(k) status. Select only cleared photopolymer liquids for denture applications. Budget for validated post-curing units if not already equipped.
Phase 2: Protocol Implementation (Weeks 5–8) Train staff on exact washing/curing sequences using calibrated equipment. Implement checklists and digital logs. Test initial batches with in-house or third-party cytotoxicity screening if desired.
Phase 3: Pilot & Validation (Months 3–6) Fabricate 15–25 cases using full protocols. Monitor patient outcomes via OHRQoL surveys and clinical exams at 1-week and 1-month follow-ups. Compare adjustment rates and comfort scores.
Phase 4: Full Integration (Months 7+) Scale to 70–100% of denture cases. Conduct quarterly internal audits of processing logs. Stay updated via FDA alerts on new clearances or recalls.
Phase 5: Continuous Improvement Participate in continuing education on ISO 10993 updates. Consider hybrid workflows for high-risk patients. Re-evaluate annually as new resins enter the market with enhanced formulations.
When protocols are followed, 3D printed resins deliver predictable safety profiles with minimal monomer-related complications. Clinics report fewer mucosal issues and higher patient satisfaction due to precise fit and reduced chair time. By 2026, FDA emphasis on validated digital workflows continues to favor compliant practices, with non-adherent operations facing regulatory and liability risks.
The transition to photopolymer resins is not inherently riskier than traditional methods—it simply demands disciplined post-processing. North American clinics that master biocompatibility and monomer control will lead in safe, efficient digital prosthetics while protecting patients and maintaining full FDA compliance.

Dry & wet milling for zirconia, PMMA, wax with auto tool changer.
learn more
High-precision 3D scanning, AI calibration, full-arch accuracy.
learn more
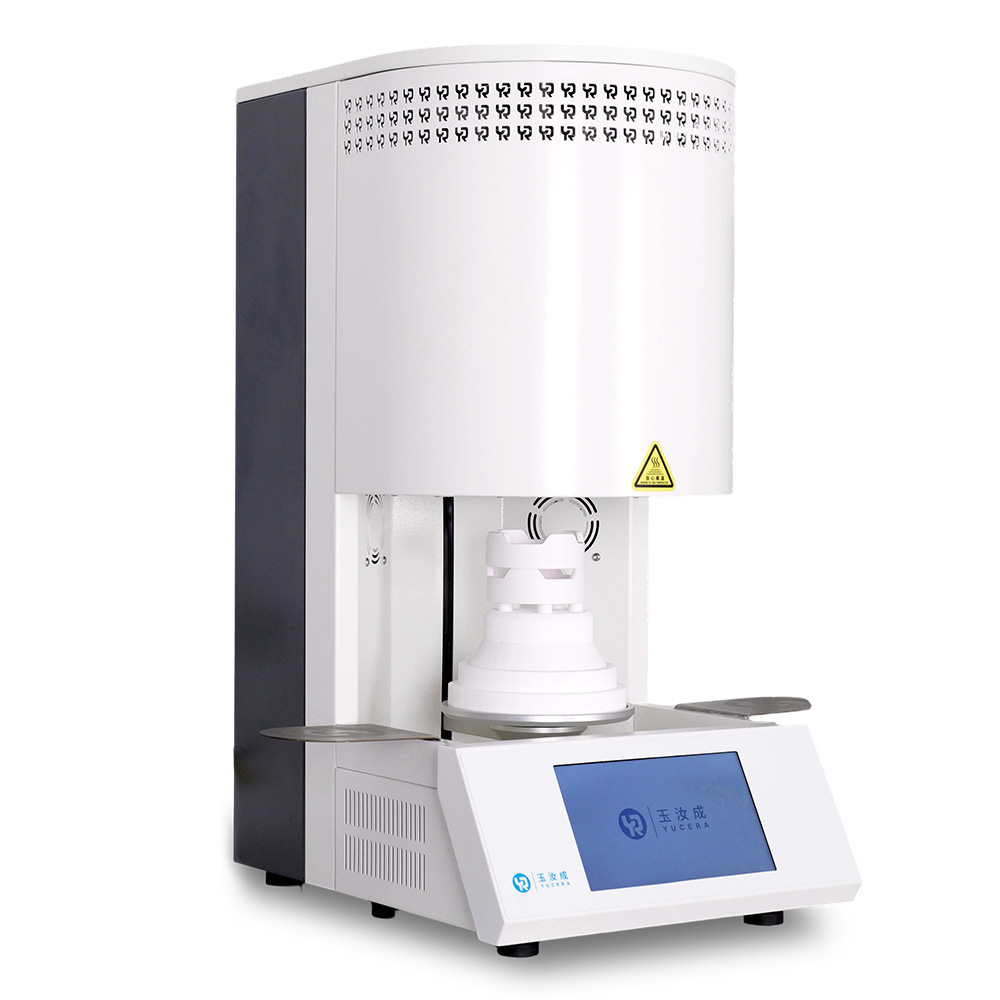
40-min full sintering with 57% incisal translucency and 1050 MPa strength.
learn more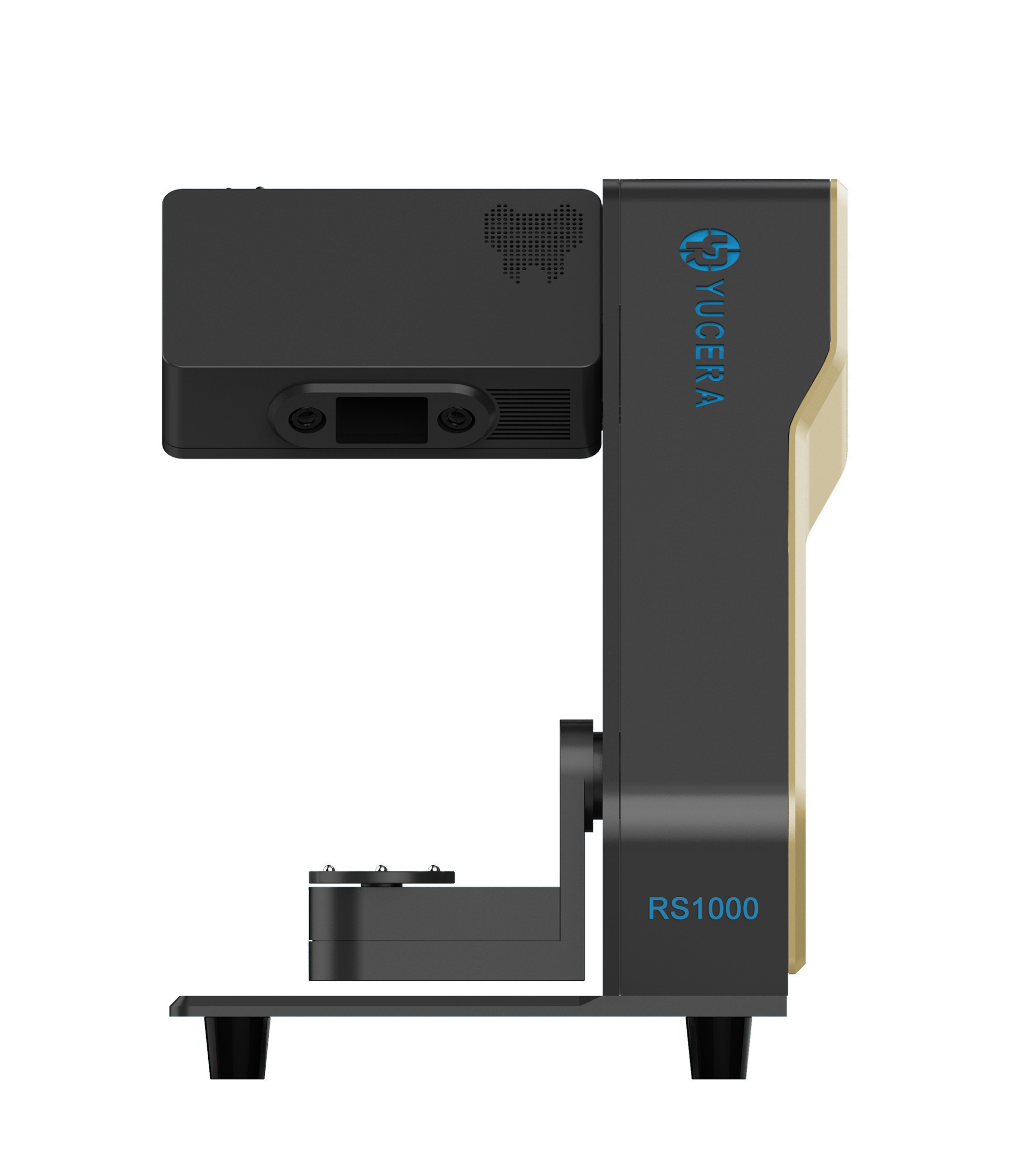
40-min cycle for 60 crowns, dual-layer crucible and 200°C/min heating.
learn more
High-speed LCD printer for guides, temporaries, models with 8K resolution.
learn more




2025-10-15

2025-11-27

2025-09-24


